Patient history
Fred, a 48 year old farm labourer, presented at his GP with a painful lesion on his tongue. A heavy smoker since the age of 16, Fred smoked a packet of cigarettes a day. He also drank six cans of beer every day, more on the weekend. The GP prescribed antifungal lozenges. When this was not effective, Fred was prescribed antibiotics.
Clinical appearance at presentation
Edentulous 48 year old with no other abnormalities other than a large erythroleukoplakic exophytic mass on the left lateral margin of the tongue extending onto the ventral surface, about 3x2cm and firm to palpation. No palpable neck nodes were observed at the time.

What the investigation showed
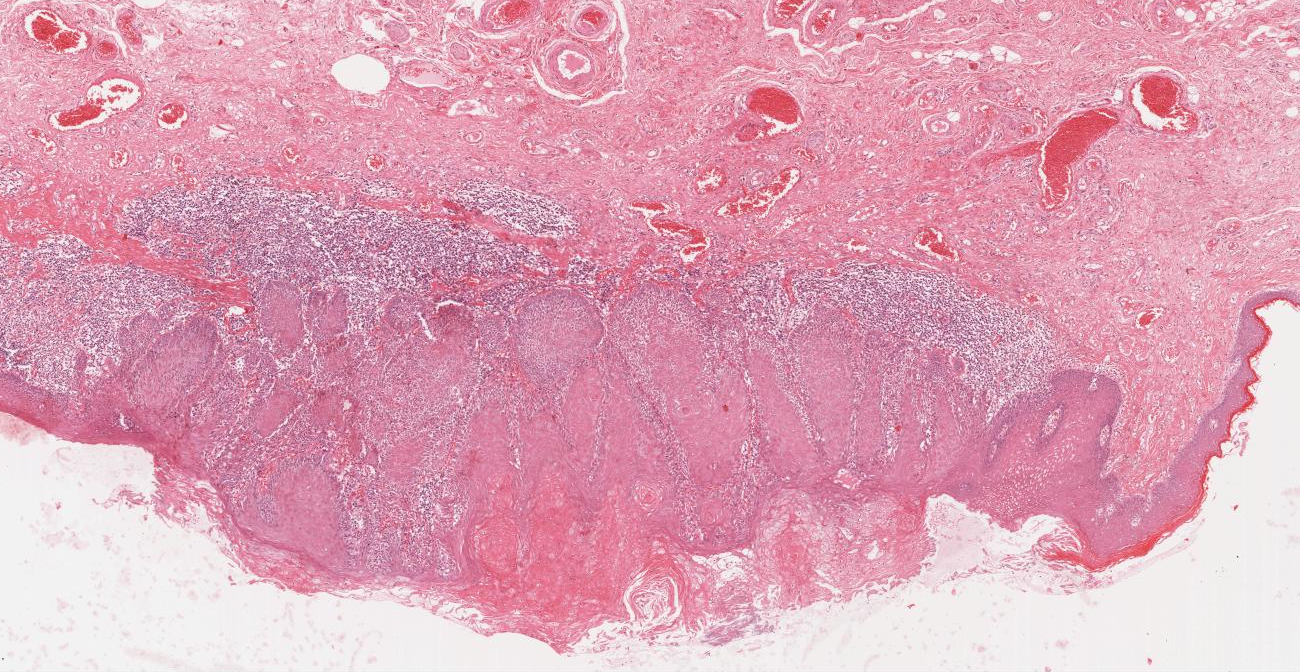
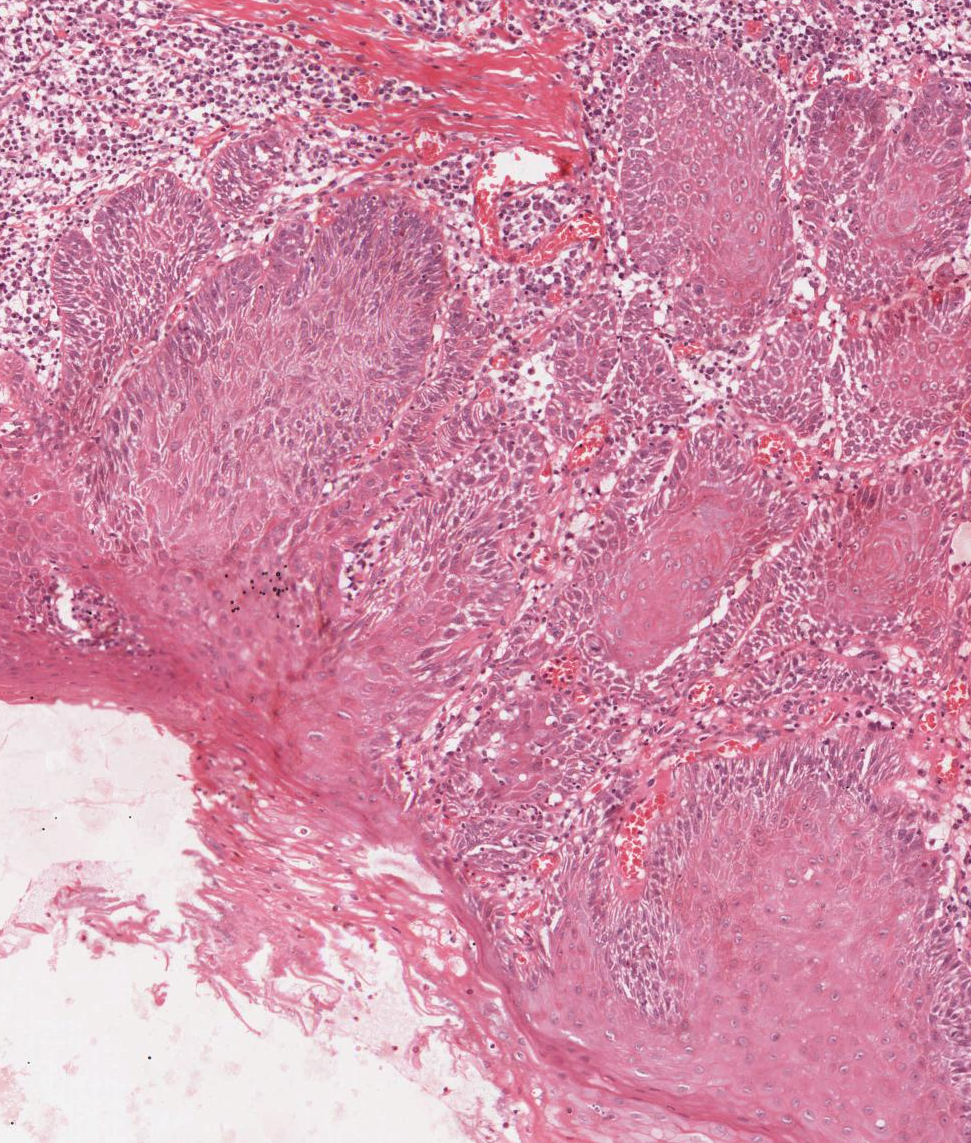
Biopsy of the lesion showed it to be a squamous cell carcinoma. Fred was referred to The Royal Melbourne Hospital’s head and neck tumour multidisciplinary clinic for definitive treatment, where his tumour was staged as T2N0M0 (stage II oral cancer).
Patient treatment and outcome
Fred’s tumour was surgically removed with concurrent elective neck dissection. Pathologically positive lymph nodes were observed, and the tumour was re-staged as T2N1(p)M0 (stage 2 oral cancer, spread to the lymph nodes). Fred underwent a full course of radiotherapy to his upper left neck over a seven-week period. Following treatment he had trouble speaking and eating, with profound xerostomia (dry mouth). An enlarged lymph node in the right side of his neck was observed at a review appointment three months later and subsequently removed.
Early the next year, Fred presented to his doctor with fatigue and a worsening cough. He had multiple lung lesions, which were eventually diagnosed as metastatic squamous cell carcinomas.
Fred died in July that year, 13 months after his initial diagnosis.
Key learning from this case study
- Smoking and alcohol consumption are significant risk factors for squamous cell carcinoma of the tongue.
- Many people at higher risk of oral cancer, including those who smoke or drink regularly, do not receive regular dental examinations. However, comprehensive oral examination and regular dental care is even more necessary for these patients to prevent or detect oral cancer earlier.
- Late presentation is quite common. Unfortunately, once oral cancer has spread to the lymph nodes prognosis significantly declines. Treatment is likely to entail major surgery, complex reconstruction and adjuvant radiotherapy or chemoradiotherapy, with severe functional impairment for survivors.
- Patients whose tumours are stage I or 2 may have excellent cure rates with minor surgery and few aftereffects. However, as in Fred’s story, this is not always the case. The earlier oral cancer is detected, the more likely that treatment will be effective with improved survival.
This case study is based on a real case report. Names and identifying details have been changed to protect the privacy of individuals. It was written by Michael McCullough, Professor of Oral Medicine, University of Melbourne Dental School.